Yale Psychiatric: the Tragic Case of Father John Ward (Faith: the Unholy Trinity)
ORIGINALLY WRITTEN: January 2023
DISCLAIMER: I am not a psychiatric professional. I do have a degree and spent years studying the intersection between the mental health and correctional systems, but I am not a clinician or an individual with a lot of clinical knowledge.
CONTENT WARNINGS: Psychiatric Abuse
As of writing this post (January 2023), there are five notes regarding John's admission to Yale Psychiatric after the failed exorcism of Amy Martin. I'm going to transcribe them in order of events, and not in the order they are found. The first note we would see examining John's case file, if he were an actual patient, would be the intake assessment form:
Yale Psychiatric Institute NEW PATIENT INTAKE FORM
Patient Name: Ward, John Thomas
Age: 33 Sex: M Ethnicity: White/Caucasian
Assigned Counselor: Spinel, James, PhD
Health Examination Results: Height: 6 feet 2 inches Weight: 185 lbs HR: 92 bpm Blood Pressure: 135/81
Current Status: Minor cuts and bruises, sprain in left ankle.
Patient is in a state of psychologic shock.
Existing Conditions:
Asthma (dormant) Diminished mobility from childhood injury to right knee.
Notice the little note there about psychologic shock. We do get elaboration on the comment made by whoever conducted the intake process, which come from Yale Psychiatric Notes 1 & 2:
Notes - new patient initial consultation
Subject: John Thomas Ward
Present: Dr. James Spinel, PhD, and two orderlies
Subject non-responsive for first half-hour, followed by fragmented 'exorcism' narrative
Subject unable to maintain consistency in story (for example, stating that Amy was in the basement and then saying she was in the attic)
Subject insists incident was the result of demonic possession
Cannot declare subject of sound mind; will require several more sessions to fully understand subject's mental state. Will advise Martin Family attorneys.
—
Subject is suffering from delusion. In John's mind, he plays the role of the hero sent by God to protect the innocent. In order to escape the consequences of his actions, he has created his own reality. In order for everything to make sense, he needs to believe in the evil spirits and paranormal occurrences. I recommend an in-vivo approach until we can get John to accept the truth.
And for the love of God, please have Ms. Martin transferred to another facility. Somehow, John knows that she is in here with him.
Then there's the newer documentation and references to In Vivo, found in the GOODIES folder of the game. See the text around bullet point 3.
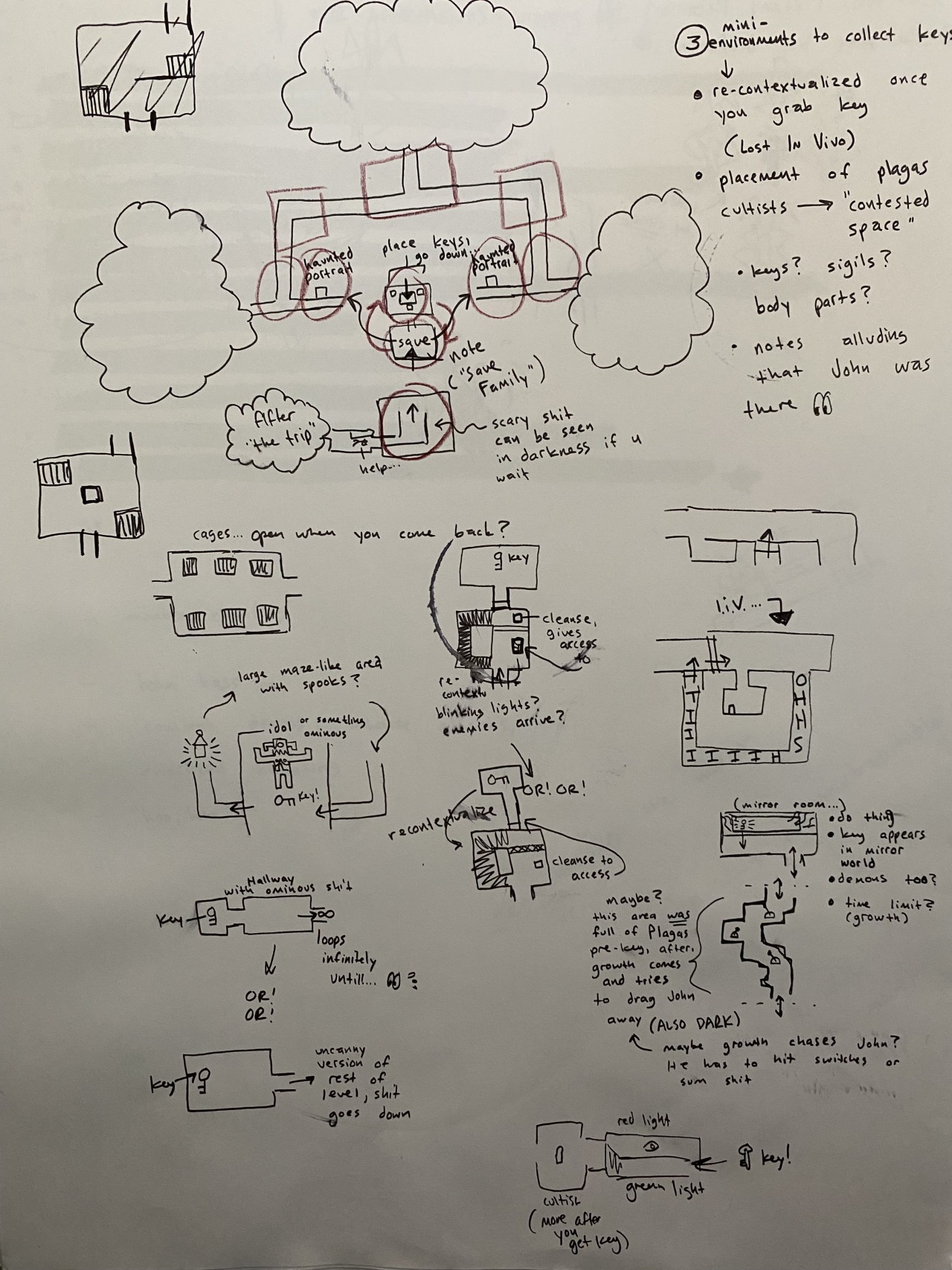
[IMAGE DESCRIPTION: An image of development notes for Faith: The Unholy Trinity Chapter 3, which were taken in an non-lined notebook. There are several roughly drawn images of the page, consisting of level mapping for puzzles in what the developer has called, in previous notes, GaryLand. The text beside bullet point 3 reads "Mini-environments to collect keys. Re-contextualized once you grab key (lost In Vivo). Placement of plagas cultists is 'contested space'. Keys? Sigils? Body parts? Notes alluding that John was there". Beside the last note is a doodle of the eyes emoji, with two stylized eyes looking to the left toward the text. END DESCRIPTION.]
Here's the thing about psychiatric institutions: They suck.
The mental health system in modern day America is better than it was in the 80s, naturally, but not by much. It is important to note that the deinstitutionalization of the mental health system was the right call to make. However, I must note that the lack of funding and resource allocation (mostly due to greed among politicians and public perception of those with mental illness) made it so that individuals are still institutionalized. As of the modern era, individuals with mental illness are disproportionately incarcerated.
The Prison Policy Initiative has a wonderful online research library with up-to-date and reflective research on the rates and treatment of individuals incarcerated, as well as how current carceral practices only work to exacerbate these issues through intensive focus on punishment:
Mental HealthBut traveling back in time, before the tides shifted, we have to understand what the environment was like within psychiatric wards/asylums.
The deinstitutionalization of mental health emerged in the 50s following World War II. To make a very long story short, the human rights abuses were put into the spotlight. Several factors, such as inhumane living conditions, harmful treatment practices (which we will elaborate on later), and the rising costs and demand for psychiatric treatment, all contributed to the call for deinstitutionalization. The goal was to improve the quality of life for people with mental illness, and to really just… allow them to exist as humans within society. Though the movement began in the 50s, it didn't gain much popularity among advocate groups until the 60s and 70s (e.g., the National Alliance on Mental Illness (NAMI) and Project Release), where the movement truly took off.
However, large-scale closures of institutions didn't actually happen until the 80s, at least in the States. This means that, come 1986/1987, there were still institutions actively running. If you'd like to read more about how psychiatric institutions were run in this era, then I highly recommend reading Dr. David Laing Dawson's personal testimonies as a clinician during the era of asylums and advocacy:
The Decline of Mental Illness Treatment from the 1980s OnBut what were popular treatment modalities for patients like John? Firstly, and mentioned in the in-game notes, we have In Vivo Exposure Therapy, or more simply put: Exposure Therapy.
The American Psychiatric Association, in their Clinical Practice Guideline(s) for the Treatment of Posttraumatic Stress Disorder (2023), define In Vivo Exposure as:
Directly facing a feared object, situation or activity in real life. For example, someone with a fear of snakes might be instructed to handle a snake, or someone with social anxiety might be instructed to give a speech in front of an audience.
This intervention is not limited to PTSD, though, and is often used for other clinical concerns such as phobias, panic and anxiety, and (in some cases) Obsessive-Compulsive Disorder. The ultimate goal is to break the pattern of avoidance while confronting the fear in a safe environment. Which is great… for patients who are ready to confront these things. If there's one lesson to take away from this post, it's that treatment cannot be forced. Treatment is ineffective if the person requiring it is non-consenting or otherwise unwilling/unable to go through the modality.
So when you look at a patient like John, who is in an active state of crisis, and decide the best treatment intervention is to (effectively) tell him to "Suck it up" and induce anxiety and fear? It's disgusting and it would, in a realistic scenario, only exacerbate his symptoms even further. Which it seems to do, if the line about John having a reaction to Amy's presence in Yale Psychiatric is anything to go by. The man believes she is possessed by a demon (or knows she is), and has intense dread and anxiety around trying to save her (to the point where it's already a fixation). Exposing him to Amy's presence, or even the possibility of it, is not going to do him well until he is guided down from a crisis state and able to understand what is going on (as well as process the events that took place in the Martin home, because Amy would be a psychological trigger of recollection for said events).
John's official diagnoses are, ultimately, mild anxiety and acute coulrophobia (aka: fear of clowns). This much is clarified in the release form:
RELEASE FORM
SUBJECT: John Thomas Ward
DOR: 31 Oct 1986
This form certifies that the subject is hereby released from my care after having completed their required counseling and treatment to my satisfaction, with confidence that they are ready to resume their normal daily activities as a mentally stable member of society.
Dr. James Spinel, PhD
EXISTING CONDITION:
Mild anxietyAcute coulrophobia
As an aside, can we just point out how John was only admitted for a month, give or take some days? Even if we take the events at face value (aka: demons are real; Hell is real; Lucifer is planning an invasion of Earth to reclaim what God has taken from him-), this feels… entirely too short to state that John is fully recovered.
At least from my interpretation of the intent behind "a mentally stable member of society", as the stigmatization of mental illness would place the burden of showing minimal, if any, signs of distress within day to day life… unless you were a hard-working husband who drank off most of his time at home while beating his wife, lest we forget the nuclear family values and toxic masculinity that still run rampant in American society. But I digress...
And immediately bring your attention to a bit of a continuity issue that, effectively, renders my last point moot: John's letter to Dr. McGlashan, who we can assume is a director of sorts within Yale Psychiatric.
This note is dated for December 30th, 1986:
Dear Dr. McGlashan,
It has been thirty days since the beginning of my treatment here at Yale Psychiatric Institute. Dr. Spinel, who has been so patient with me, has helped me understand my afflictions and has helped me fund a way to move forward and accept the truth.
With Dr. Spinel's help, I have come to accept what really happened in September at the Martin family residence. I accept that what happened was not the result of any supernatural phenomenon, but rather the desperate actions of a young girl driven to violence by her dogmatic parents and old church rituals that are thought to drive out evil.
I am happy to report that, since accepting the truth, my nightmares have ceased and I now enjoy peace of mind that I have not felt since the incident. Given my progress since first coming here, I respectfully request my release from Yale Psychiatric Institute, contingent upon follow-up appointments with Dr. Spinel in the future.
Sincerely,
John Ward
And raises several questions, such as:
- If the failed exorcism took place in September, does this mean that John was within Yale Psychiatric from September to December?
- Why was there a release form authorized in October 1986 by Dr. Spinel?
- John states, "It has been thirty days since the beginning of my treatment […]". Does this mean that there was a second admission period between October and December?
- If there was, when did that occur? Was he brought back in during the last weeks of October? In November?
My personal belief is that John was institutionalized twice. Once immediately following the failed exorcism, and once more after due to a relapse (hence the specification "[…] contingent upon follow-up appointments with Dr. Spinel in the future."). John, by this point, is aware of his mental health concerns and acknowledges that he needs more in regard to his treatment. Here, he's showing a clear capacity to establish and (hopefully) follow a community treatment regiment.
And this is where a bibically-accurate, canonical analysis, would end. A bit of insight into what happened, why it happened, and the ramifications (albeit brief). But here's the thing:
I believe there's more to John's case, since I believe in the blending of two prominent theories (everything is real versus everything is imagined). Personally, based on these notes and a few key dialogs within Chapter 3, I believe that John (in addition to the Anxiety) experiences Psychosis brought on by Paranoid Schizophrenia. In context of the game's plot, he experiences Persecutory and Grandiose Religious Delusions.
Let me explain.
There are several types of delusions, and the severity of these delusions can vary from individual to individual. More on the specifics (as well as recommended treatment modalities) can be found in this PDF.
Generally speaking, though, the types of delusions I mentioned are described as follows:
- Grandiose: An individual experiences an exaggerated sense of importance, power, knowledge, or identity, that may have some type of theme.
- Persecutory: An individual is fixated on the prospect of being attacked, harassed, persecuted, or conspired against.
Sounds familiar, yeah? Let's break it down:
- Grandiose: Exhibited in all chapters. John is of the belief that he is a destined savior to Amy Martin. That he is the only one who can save her from the demon(s) plaguing her because he is the only one with the power and ability to do so. He, in the Super Miriam boss fight, also claims to have God's power directly within him. That he, in a way, is God (at least, in that moment).
- Persecutory: Exhibited in all chapters, prominent in Chapter 3. In Chapter 1, there's "The Offering" Ending. John is (or perceives to be) stopped in the middle of the road home by Gary and his cult. Then, in Chapter 3, the entire arc around Gary's cult centers around the idea of John being persecuted (targeted by the cult for his attempts to save Amy).
One thing that slates me toward this conclusion is the brief mention of John's mother, Meredith. Amy's demon taunts John by asking him "What about Meredith? Did she get better?" and says how he couldn't save her. And based on the delivery of this line, it's clear that some sort of illness was what killed Meredith. Given that Schizophrenia in of itself typically doesn't cause death (though symptoms can contribute to other factors, such as poor physical health, risk-taking behaviors, higher risks of suicide), we have to look beyond the mental health aspect for a brief moment.
According to fairly recent research, there have been connections made between an individual's Schizophrenia diagnosis and their likelihood for developing Alzheimer's Disease. Kochunov et al. (2020) state:
"Schizophrenia (SZ) is a severe psychiatric illness associated with an elevated risk for developing Alzheimer’s disease (AD). Both SZ and AD have white matter abnormalities and cognitive deficits as core disease features. […] SZ and AD have diverse etiologies and clinical courses; our findings suggest that white matter deficits may represent a key intersecting point for these 2 otherwise distinct diseases. Identifying mechanisms underlying this white matter deficit pattern may yield preventative and treatment targets for cognitive deficits in both SZ and AD patients."
Now, as a personal note, I have seen and experienced what Alzheimer's can do to people and how long of a process it is. My maternal grandfather, tragically, passed due to the illness in 2020. I still cannot discuss the symptomatology and progression in full as a result of the grief, but I can direct attention to the Alzheimer's Association and their article on the stages of progression:
Stages of Alzheimer'sReturning to the psychoanalytical aspect, mental illness can be hereditary and passed down, in addition to being individually developed (through whatever means, which are often referred to as the biopsychosocial factors of development). Such is true with the case of Schizophrenia.
Additionally, there does seem to be evidence suggesting that John's perception of events is questionable. Of course, I must note here that every character in this story is an unreliable narrator. Every character has their motives in the information they share and how they share it. This is in no way, shape, or form, me saying that other characters are objectively right in their perceptions. Especially Gary.
Gary is a cult leader. Even if the cult is not as dramatized as they appear to be (e.g., they are not, in fact, kidnapping babies and sacrificing people)… he is still running a cult. He is still capable of being manipulative regardless. I can absolutely delve into the psychology and structure of cults, but this post is long enough as is.
So instead, let's look at what it is Gary says to contradict John's point of view. The primary dialog that I believe points us to a faulty perception is Gary's recollection of the Martin twins:
"Oh, John… deep down, you always knew the twins were an illusion. But you could not resist chasing after lost (hurt) souls. I suppose you wished they were real, just like the late Mrs. Martin. That is how I knew you would come to me."
The popular analysis among the fandom is that Mrs. Martin miscarried the twins, and experienced a rough patch of grief surrounding the event. Again, I have seen similar experiences in my personal life, so I can sympathize with and affirm how rough this process can be. This is why Mrs. Martin had put effort into the belief that they were still expected/born, with the room being set up for them and the crib being discarded in the Martin's basement (as well as the birthday party and clown aspect).
John knew this at the time of exorcising Amy, but his own mental break altered his perception of events and made him believe in the same narrative that Mrs. Martin presented: The twins were alive. The difference here is that John tied the twins into his perception of the game's events, and came to the conclusion that Gary (and his cult) kidnapped them for ritualistic reasons.
Likewise, a lot of Gary's dialog has key words switched out. A list of these words is as follows, with their substitutions in parentheses:
- enter (abuse)
- lost (hurt) souls
- Vessel (Victim)
- journey (despair)
Again, this could be a simple nod to Gary's capacity for manipulation as a cult leader. But that doesn't exclude it from also pointing out John's perception of the series' events. In fact, this could be John's psyche interjecting and affirming itself.
So, if John does have this diagnosis, what would a thorough treatment modality look like if they'd pinpointed it back then? If he was institutionalized a third time, after stopping the Profane Sabbath?
The answer to that is either Insulin Shock Therapy (IST)/Insulin Coma Therapy (ICT), or Chlorpromazine (a strong antipsychotic medication).
It's important to note here that IST/ICT fell out of favor in the 1960s, like most shock therapies (with the exception of electroconvulsive therapy). Jones (2000) details the history and modality of ICT, stating:
"Comas were induced on five or six mornings a week. Typically, the third dose of insulin was 10±15 units with a daily increase of 5±10 units until the patient showed severe hypoglycemia. Treatment continued until there was a satisfactory psychiatric response or until 50±60 comas had been induced. Experienced therapists let patients spend up to 15 minutes in 'deep coma' with hypotonia and absent corneal and pupillary reflexes. Clinicians noted gross variation between individuals in response to a given dose of insulin. Also, in the course of treatment a patient could show day-to-day variation in his reaction. Further there was an uncertain relationship between clinical signs and the blood glucose level. The hypoglycemia made patients extremely restless and liable to major convulsions. Comas were terminated by administration of glucose via a nasal tube or intravenously."
If any of this sounds vaguely familiar, it's because the treatment modality was highlighted in the story of John Nash, a fundamental American mathematician with Schizophrenia.
The 2001 film A Beautiful Mind showcases Nash's story, including the usage of ICT. Attached is a video clip from the film, which contains content that may be triggering/disturbing. Watching it is not vital to this analysis, as it's to illustrate the paragraph above:
Ultimately, the takeaway is this:
- Mental illness plays a huge role in the game's overarching narrative, even if not considered a major plot element in of itself. The Satanic Panic was a moral panic used by fundamentalist Christians to excuse abuse within their churches, excuse the discrimination of BIPOC and queer folk, and dismiss rising concerns regarding mental health advocacy. This, alongside simply targeting youth subcultures to preserve the nuclear family imagery that arose during the previous generations.
- John Ward is easily one of the most fascinating characters to exist, in my opinion, because of how his character is linked to this idea. John Ward is a beacon (for a lack of better term) for this message within the game. He exhibits mental health issues canonically (re: the official diagnoses) and can be analyzed as having a deeper, more expansive diagnosis.
Everything I have said is interpretation, and is not entirely canon in the bibically-accurate sense. This is just a topic that's been in my mind since the release of Chapter 2's demo. You can feel free to agree or disagree with literally anything I have said, and I love hearing others' interpretations as well! The theories scattered around the fandom, are just so good. So I wanted to help contribute in some way!